 |
|
|
|
|
|
|
| Thalassemia Pregnancy
Thalassemia Minor Pregnancy Mother Thalassemia Minor
+ Father Normal
Beta-Thalassemia Minor During
Pregnancy
METHODS: A population-based study comparing all pregnancies of women with and without ß-thalassemia minor was conducted. Deliveries occurred during the years 19882002 at Soroka University Medical Center. A multivariate logistic regression model, with backward elimination, was constructed to find independent risk factors associated with maternal ß-thalassemia minor. RESULTS: During the study period there were 159,195 deliveries, of which 261 (0.2%) occurred in patients with ß-thalassemia minor. The following conditions were significantly associated with ß-thalassemia minor: oligohydramnios (odds ratio [OR] 2.1; 95% confidence interval [CI] 1.2%, 3.7%), intrauterine growth restriction (IUGR; OR 2.4; 95% CI 1.4%, 4.2%), Jewish ethnicity (OR 1.5; 95% CI 1.2%, 1.9%), and previous cesarean delivery (OR 1.4; 95% CI 1.1%, 2.0%). No significant differences were noted between the groups regarding perinatal outcomes such as birth weight, low Apgar scores, congenital malformations, or perinatal mortality. Patients with ß-thalassemia minor were more likely to have cesarean deliveries than were the nonthalassemic parturients (16.9% and 12.2%, respectively; P = .021). However, while controlling for possible confounders such as IUGR, oligohydramnios, and previous cesarean delivery, with another multivariate analysis with cesarean delivery as the outcome variable, ß-thalassemia minor was not found as an independent risk factor for cesarean delivery (OR 1.3; 95% CI 0.9%, 1.9%). CONCLUSION: The course of pregnancy of patients with thalassemia minor, including perinatal outcomes, is favorable. Because higher rates of IUGR were found, we recommend ultrasound surveillance of fetal weight for early detection of IUGR. Diet for thalassemia minor
to increase haemoglobin ?
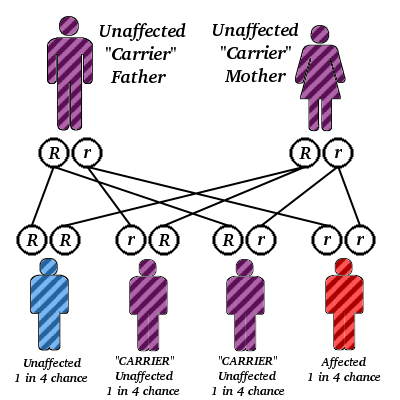
Thalassemia Minor What is the difference between thalassemia minor and major? There are two forms of beta thalassemia. They are thalassemia minor and thalassemia major (which is also called Cooley's anemia). Thalassemia minor: The individual with thalassemia minor has only one copy of the beta thalassemia gene (together with one perfectly normal beta-chain gene). The person is said to be heterozygous for beta thalassemia. Persons with thalassemia minor have (at most) mild anemia (with slight lowering of the hemoglobin level in the blood). This situation can very closely resemble that with mild iron-deficiency anemia. However, persons with thalassemia minor have a normal blood iron level (unless they have are iron deficient for other reasons). No treatment is necessary for thalassemia minor. In particular, iron is neither necessary nor advised. Thalassemia major (Cooley's anemia): The child born with thalassemia major has two genes for beta thalassemia and no normal beta-chain gene. The child is homozygous for beta thalassemia. This causes a striking deficiency in beta chain production and in the production of Hb A. Thalassemia major is, therefore, a serious disease. The clinical picture associated with thalassemia major was first described in 1925 by the American pediatrician Thomas Cooley. Hence, the name Cooley's anemia in his honor. At birth the baby with thalassemia major seems entirely normal. This is because the predominant hemoglobin at birth is still fetal hemoglobin (Hb F). Hb F has two alpha chains (like Hb A) and two gamma chains (unlike Hb A). It has no beta chains so the baby is protected at birth from the effects of thalassemia major. Anemia begins to develop within the first months after birth. It becomes progressively more and more severe. The infant fails to thrive (to grow normally) and often has problems feeding (due to easy fatigue from lack of oxygen, with the profound anemia), bouts of fever (due to infections to which the severe anemia predisposes the child) and diarrhea and other intestinal problems. What is Mediterranean anemia? The gene for beta thalassemia is not evenly distributed among peoples. It is, for example, relatively more frequent in people of Italian and Greek origin, both of which are peoples from the Mediterranean. Because of this, thalassemia major has been called Mediterranean anemia. The name thalassemia was coined at the University of Rochester in upstate New York by the Nobel Prize-winning pathologist George Whipple and the professor of pediatrics William Bradford from the Greek thalassa for sea and -emia, meaning the blood. Thalassemia means "sea in the blood." But for the Greeks, the sea was the Mediterranean, so thalassemia also conveys the idea of the Mediterrranean in the blood. The reason that the gene for beta thalassemia is relatively common, for example, among people of Italian and Greek origin is that parts of Italy and Greece were once full of malaria. The presence of thalassemia minor (like sickle cell trait in Africa) afforded protection against malaria, and therefore, this gene thrived. What is the genetic pattern of inheritance of beta thalassemia? The pattern of genetic transmission of beta thalassemia (and sickle cell disease) was deciphered by James V. Neel when he was at the University of Rochester (he later went to Michigan). Dr. Neel recognized that the parents of children with thalassemia major had thalassemia minor with one beta thalassemia gene. When these parents had children, they have a 25% chance of having a thalassemia major child (with both genes for beta thalassemia), a 50% chance of having children with thalassemia minor (with only one gene for beta thalassemia), and a 25% chance of having a child without thalassemia major or minor (with both genes for normal beta chains). This form of inheritance is medically referred to as an autosomal recessive pattern. The diagnosis of thalassemia major and minor Persons with thalassemias have smaller sized red blood cells than normals as well as low red blood cell counts (anemia). Thalassemia major and thalassemia minor can now be diagnosed (and distinguished from one another) not only by conventional clinical and blood testing, but also by molecular medical tests. These tests permit accurate diagnosis to be made at any time, even before birth (in fact, well before the beta chain machinery is fired up to make beta chains for hemoglobin). The treatment of thalassemia major Infants with thalassemia major are well at birth because of a special form of hemoglobin present in the fetus and newborn. Eventually, however, this hemoglobin is replaced by defective hemoglobin. Symptoms emerge late in the first year of life. The child develops pale skin, irritability, growth retardation, swelling of the abdomen due to enlargement of the liver and spleen (hepatosplenomegaly) with jaundice. This is associated with severe anemia with rupture of the red blood cells (hemolytic anemia). The child with thalassemia major becomes dependent on blood transfusions and, although they do help, they create further problems including iron overload. Folic acid supplementation is often given. At this time, there is only treatment for relieving the symptoms of the illness for thalassemia major. Gene therapy remains a potential treatment for the future. The long-term hope is that
thalassemia major will be cured by insertion of the normal beta-chain gene
through gene therapy or by another modality of molecular medicine.
MOST IMPORTANT, if you and your partner have thalassemia trait, you are at risk for having children with thalassemia major, a serious disease without satisfactory treatment. At the present time, the principal treatment for children with thalassemia major is regular blood transfusions. Thalassemia Trait Thalassemia trait occurs when a person inherits one thalassemia gene from one parent and a normal hemoglobin gene from the other parent. A person with thalassemia trait is well and usually unaware that he or she has the condition. Some individuals with thalassemia trait have a mild anemia but this generally does not cause symptoms. Since thalassemia is inherited, a person can pass it on to one's children. If one parent has thalassemia trait and the other parent has the normal type of hemoglobin (A) there is a 50% (1 in 2) chance with EACH pregnancy that the baby will be born with thalassemia trait. Who Is At Risk for Thalassemias?
Family History
Ancestry
Beta thalassemias most often
affect people of Mediterranean (Greek, Italian, and Middle Eastern), Asian,
or African origin or ancestry
It is quite common for people with thalassemia minor not to know they have it, because there are usually no symptoms. If you are worried that you or your husband might be a carrier, a routine blood test will establish if you have thalassemia minor. If you or your husband has thalassemia and you are planning a family or are already expecting a baby, the other parent will need to have a blood test so the risk can be assessed. Positive test results are valuable information to share with the rest of your family, who should also be tested if they are planning pregnancies. What should I do if I am pregnant and I have thalassemia? Unfortunately, you cannot do anything to reduce the risk of passing thalassemia to your baby. However, if you have a milder form of thalassemia, there is a very good chance that you will have a healthy pregnancy. If you have thalassemia minor you might be more prone to iron deficiency (anemia) during pregnancy. However, beta thalassemia can affect blood test results during pregnancy, causing them to indicate that your iron stores are low when they are not. As a result, if you have beta thalassemia, you should have additional blood tests to confirm that you are iron-deficient before you take iron tablets. If you do become anemic, you will need to take iron supplements. If you have thalassemia, you will also benefit from taking 5mg of folic acid a day. Even women with the more serious beta thalassemia major are able to have healthy pregnancies, if the condition has been well treated. If you have been taking drugs to prevent the build up of iron, these should usually be stopped during pregnancy. Talk to your doctor about thalassemia and your pregnancy. How do I find out if my unborn baby has thalassemia? If you or your husband have been diagnosed with thalassemia minor, there are three ways to find out if your baby has inherited it. Chorionic villus sampling (CVS): This involves taking a small sample of the placenta for DNA testing at about 10 to 12 weeks of pregnancy. Amniocentesis: The amniotic fluid surrounding your baby is tested at between 15 and 18 weeks of pregnancy. Percutaneous umbilical blood sampling (PUBS): A blood sample is taken from the umbilical cord at about 18 to 21 weeks of pregnancy. This test is the least common and usually only used if the pregnancy is more advanced or when the results of the other tests are inconclusive. If you are concerned that your baby may have thalassemia, getting a diagnosis as early as possible in your pregnancy will give you and your husband time to prepare yourselves. |
|
||||
 |
|
|
|
|
|
| Privacy Policy for LiveIndia.Com |
Multi Dimensional Entertainment magazine from INDIA |
 |








